Most essential systems are built around density. More people usually justify more services, more investment, more access. That logic works well in cities, where proximity and scale make everything more efficient.
But rural Wisconsin doesn’t work that way. And neither does healthcare.
A System That Still Follows Density
Large parts of Wisconsin are defined by low population density, small towns, long travel distances, and uneven settlement patterns. This creates a problem many systems aren’t designed to solve.
You can’t rely on clustering. You can’t rely on proximity. And you can’t assume another option is nearby.
Yet unlike Kwik Trip, hospitals don’t adjust to those constraints in the same way. They remain concentrated.
The Pattern Is Exactly What You’d Expect
If healthcare followed coverage instead of density, hospitals would be distributed broadly across the state, filling gaps between towns and along rural corridors.
But they aren’t.
Across Wisconsin, hospitals are concentrated:
- in Milwaukee and Madison
- in regional cities
- along major population centers
This isn’t a scattered pattern. It’s systematic. Hospitals don’t build coverage. They follow demand.
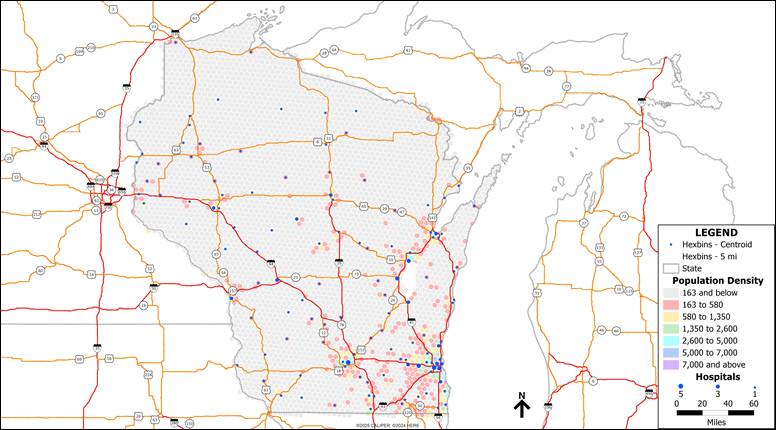
Map #1 – Healthcare Follows Density: Hospital Locations vs Population
What Matters Isn’t Where Hospitals Are, It’s How Far Away They Are
Location maps can be misleading. In rural areas, access matters more than presence. When you shift the analysis to drive time to the nearest hospital, the structure of the system becomes clearer.
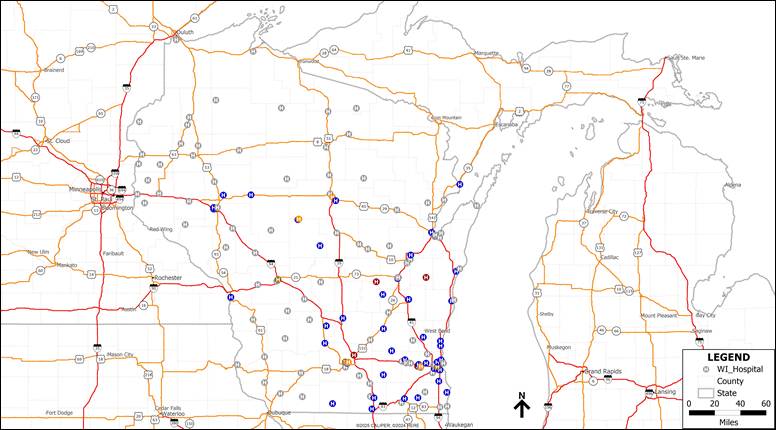
Map #2 – A Concentrated System: Hospital Locations Across Wisconsin
Across much of Wisconsin:
- access stretches beyond 10–15 minutes
- gaps are larger and more continuous
- distance becomes a defining constraint
This is the key difference:
- Retail systems can optimize for proximity
- Healthcare systems often optimize for efficiency
Hospitals are doing the latter and doing it consistently.
Why That Changes What “Access” Means
Once a system concentrates instead of distributes, the role of each location changes. In cities, hospitals are abundant. In rural areas, they become distant. That distance changes how the system functions.
Care isn’t just about availability, it’s about reach.
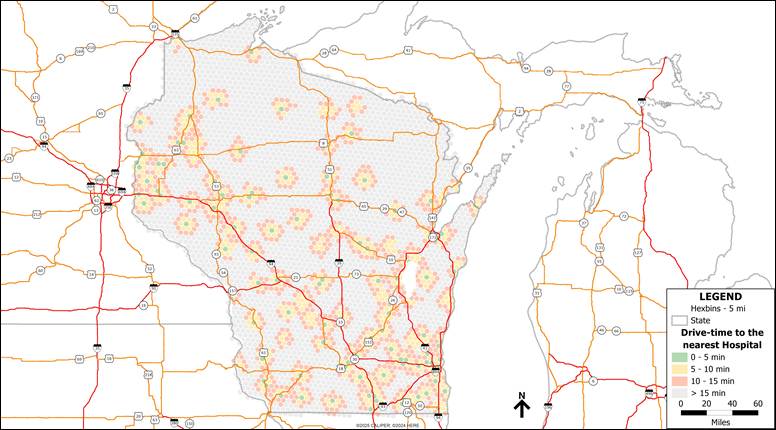
Map #3 – Distance Defines Access: Drive Time to the Nearest Hospital
The System Works, But It Solves a Different Problem
Hospitals operate under constraints that retail does not:
- high fixed costs
- staffing limitations
- specialization requirements
- regulatory barriers
You can’t place them everywhere. So instead of minimizing distance, the system accepts it. That works for efficiency. It works less well for proximity.
What This Tells Us
Hospitals in rural Wisconsin aren’t failing. They function exactly as designed. But the design is different.
Where Kwik Trip prioritizes:
- coverage over clustering
- proximity over density
- consistency over variety
Healthcare prioritizes:
- efficiency over coverage
- concentration over proximity
And in doing so, it creates a different kind of gap.
What Comes Next
Kwik Trip shows what happens when a system is designed for rural reality. Healthcare shows what happens when it isn’t. That raises a harder question: Not where services are located, but how they’re designed to serve.